Surveillance of viral diarrhea among hospitalized children in Urumqi, 2010
Sabiremu Tuohetamu, Ayiguli Yerhali, LIU Hong-bin, WU Yue-wen, LI Xin-lan
Xinjiang Uighur Autonomous Region Center for Disease Control and Prevention, Urumqi 830002, Xinjiang, China
Abstract
Objective To understand the etiological characteristics of hospitalized children with diarrhea in Urumqi. Methods Stool samples were collected from 379 hospitalized children with diarrhea in Urumqi from January to December 2010 to conduct etiological detection with ELISA, RT-PCR and PCR respectively. Results Among the 229 (60.4%) samples collected, the detection rate was 45.6% for rotavirus, 14.2% for norovirus, 4.2% for astrovirus, 3.2% for adenovirus and 1.1% for sapovirus. Co-infections were detected in 26 cases. The most common type was co-infection of rotavirus and norovirus, accounting for 50.0% (13/26). The incidence peaks of rotavirus infection occurred during January-March and October-December respectively, and the incidence peak of norovirus infection occurred in October. The children with rotavirus infection were younger than those with norovirus infection (P=0.002). All adenovirus and sapovirus infections occurred in children aged<2 years. Conclusion Rotavirus was the most prevalent pathogen of childhood viral diarrhea in Urumqi in 2010, followed by norovirus. Co-infection was detected too, to which close attention should be paid in future epidemiological and etiological researches.
2010年乌鲁木齐市住院儿童病毒性腹泻监测结果分析
沙比热木·托合塔木, 阿依古丽·伊尔哈力, 刘红斌, 毋跃文, 李新兰
新疆维吾尔自治区疾病预防控制中心, 新疆 乌鲁木齐市 830002
摘要
目的 了解乌鲁木齐市住院儿童病毒性腹泻的流行现状。 方法 2010年1-12月采集乌鲁木齐市379例腹泻住院患儿粪便标本,用酶联免疫吸附试验(ELISA)、反转录-聚合酶链反应(RT-PCR)和聚合酶链反应(PCR)检测5种常见腹泻病毒。 结果 229份(60.4%)粪便标本检出至少1种病毒。轮状病毒、诺如病毒、星状病毒、肠道腺病毒和札如病毒检出率分别为45.6%、14.2%、4.2%、3.2%和1.1%。混合感染共26例,以轮状病毒和诺如病毒组合占首位(50.0%,13/26)。1-3月和10-12月是轮状病毒流行高峰期;诺如病毒流行主要发生在10月。轮状病毒感染平均年龄小于诺如病毒感染平均年龄(P=0.002),肠道腺病毒和札如病毒感染全部发生于<2岁儿童。 结论 轮状病毒仍是2010年乌鲁木齐市儿童病毒性腹泻的最主要的病原体,其次是诺如病毒;混合感染占一定比例,在以后的流行病学及病原学研究中应该更加关注混合感染的出现。
内容大纲
本研究严格按照《全国病毒性腹泻监测方案(2007年修订版)》的要求,于2010年对乌鲁木齐市5岁以下住院患儿病毒性腹泻开展监测,以掌握本地区病毒性腹泻的流行病学特点、主要病原及其变异特征,并为我国制订有针对性的预防控制措施提供科学依据。现将监测结果分析报告如下。
1 材料与方法
1.1 资料来源 2010年1-12月,乌鲁木齐儿童医院379例5岁以下腹泻住院患儿作为研究对象,其中男性223例,女性156例,男女性别比为1.43 ∶ 1,平均年龄(11.5±9.8)月龄。腹泻诊断标准为:每日排便3次或以上,且粪便性状有改变(呈水样便、稀便等)。按照《全国病毒性腹泻监测方案》设计的统一的腹泻病例个案表,收集监测病例的病例一般资料、发病、就诊与治疗等信息,并对每位患者采集1份粪便标本。标本加标本处理液(PBS液)按1 ∶ 10比例稀释后,静置10 min,再以8000 r/min离心5 min,最后留取上清储存在-20 ℃备用。
1.2 核酸的提取
取200~400 μl处理好的粪便标本上清液,使用台湾Geneaid 公司生产的商品化核酸提取试剂盒进行病毒核酸提取,操作方法详见试剂盒说明书。
1.3 检测方法
采用酶联免疫吸附试验(ELISA)检测RV抗原,检测试剂盒购自DAKO公司,操作步骤详见试剂盒说明书。采用反转录-聚合酶链反应(RT-PCR)方法检测粪便标本中的NV、SaV和AstV,采用聚合酶链反应(PCR)方法检测AdV,所用引物及实验操作步骤严格按照《全国病毒性腹泻监测方案》要求执行。最后将扩增产物进行1.5%琼脂糖凝胶电泳,紫外灯下观察和照相,然后与DNAmarker对照,根据目的条带的大小判断结果。
1.4 统计学分析
采用EpiData软件录入数据,利用SPSS 17.0和Excel软件进行统计学分析,依据数据特征分别采用两独立样本t检验和χ2检验分析。检验统计采用95%可信区间(P=0.05),P<0.05为差异有统计学意义。
2 结果
2.1 病原检出情况 379例腹泻患儿粪便标本中229例(60.4%)至少检出一种病毒,其中属于单病毒感染203例(88.6%),混合感染26例(11.4%)。RV是引起儿童腹泻最主要的病毒,检出率为45.6%(173/379),NV位居第2位(14.2%,54/379),AstV、AdV和SaV检出率较低,见图1。混合感染包括5种两两混合感染组合,其中以RV与和NV组合占首位(50.0%,13/26),见表1。未发现3种或3种以上病毒混合感染的情况。
图1 2010年乌鲁木齐市5岁以下腹泻住院儿童病毒性腹泻病原检出情况
Figure 1 Detection rate of viral diarrheal pathogens in hospitalized children in Urumqi,2010
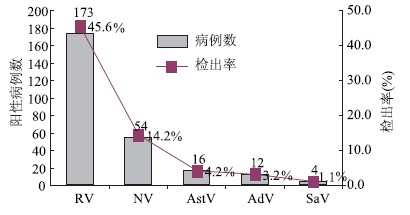
表1 乌鲁木齐市5岁以下腹泻住院儿童5种腹泻病毒混合感染情况
Table 1 Co-infection rate of 5 viral diarrheal pathogens in hospitalized children in Urumqi,2010
| 组合类型 | 阳性数 | 构成比(%) |
| RV+NV | 13 | 50.0 |
| RV+AstV | 5 | 19.2 |
| NV+AdV | 4 | 15.4 |
| RV+AdV | 2 | 7.7 |
| NV+AstV | 2 | 7.7 |
| 合计 | 26 | 100.0 |
2.2 季节分布
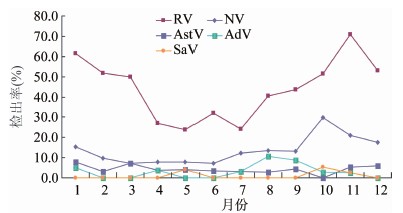
RV发病高峰主要集中在秋冬季节(10月至次年3月),高峰期检出率和其他月份相比,差异有统计学意义(χ2=15.082, P=0.000),见图2。NV全年各月均有发病,10月为发病高峰期(29.7%)(χ2=7.058, P=0.007)。16例AstV病例散在分布于除10月以外的各月。AdV在8、9月似有一发病小高峰,但和其他月份之间差异无统计学意义(P>0.05)。4例SaV病例分布如下:5月1例(4.0%)、10月2例(5.41%)和11月1例(2.63%)。
图2 2010年乌鲁木齐市病毒性腹泻各病原分月检出率
Figure 2 Monthly detection rate of viral diarrheal pathogens in Urumqi,2010
2.3 阳性病例的性别和年龄分布特征
229例阳性病例中,男、女性阳性检出率分别为58.30%(130/223)和63.50% (99/156),差异无统计学意义(P=0.312),任一病原男、女性检出率之间差异均无统计学意义(P>0.05)。7~12月龄患儿感染腹泻病毒检出率最高(χ2=10.272,P=0.001),见表2。RV感染平均年龄为(9.5±4.4)月龄,比NV平均年龄(12.3±9.6)月龄低(P=0.002)。RV在7~12月龄组患儿中检出率(53.90%)最高,与其他年龄组相比,差异有统计学意义(χ2=9.387, P=0.002)。NV以7~12月龄组检出率(16.10%)最高,但和其他年龄组比较差异均无统计学意义。AstV感染平均年龄为(11.8±9.4)月龄,各年龄组检出率差距较小。AdV和SaV感染平均年龄分别为(7.4±3.5)和(12.0±4.5)月龄,且全部发生于2岁以下儿童,见表2。
表2 2010年乌鲁木齐市病毒性腹泻住院患儿性别与年龄分布
Table 2 Gender and age distributions of the hospitalized children with viral diarrhea in Urumqi,2010
| 病原类型 | 性别 | 农村 | 合计(1) | |||||||||||||||||
| 男性(N=223) | 女性(N=156) | 0~(N=103) | 7~(N=180) | 13~(N=76) | 25~60(N=20) | (N=379) | ||||||||||||||
| 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | 阳性例数 | 检出率(%) | |||||||
| RV | 101 | 18.50 | 48 | 18.20 | 41 | 39.80 | 97 | 53.90 | 30 | 39.50 | 5 | 25.00 | 173 | 45.65 | ||||||
| NV | 64 | 11.70 | 38 | 14.40 | 13 | 12.60 | 29 | 16.10 | 10 | 13.20 | 2 | 10.00 | 54 | 14.20 | ||||||
| AstV | 2 | 0.37 | 2 | 0.76 | 3 | 2.90 | 10 | 5.60 | 2 | 2.60 | 1 | 5.00 | 16 | 4.20 | ||||||
| AdV | 5 | 0.91 | 5 | 1.89 | 5 | 4.90 | 6 | 3.30 | 1 | 1.30 | 0 | 0.00 | 12 | 3.20 | ||||||
| SaV | 17 | 3.11 | 6 | 2.27 | 0 | 0.00 | 3 | 1.70 | 1 | 1.30 | 0 | 0.00 | 4 | 1.10 | ||||||
| 合计 | 130 | 58.30 | 99 | 63.50 | 57 | 55.30 | 124 | 69.90 | 44 | 57.90 | 4 | 20.00 | 229 | 60.40 | ||||||
2.4 混合感染分布特征
本次监测发现混合感染病例26例,检出率为6.9%,男女性别比为1.9 ∶ 1。年龄范围在1~16月龄,其中92.3%(24/26)的病例年龄在1岁以下,无明显的季节分布特点。
3 讨论
为更全面掌握乌鲁木齐市病毒性腹泻的病原谱,本研究对引起本地区5岁以下住院腹泻患儿病毒性腹泻的常见病原及其混合感染情况进行了系统监测。结果60.40%(229/811)的病例至少检出一种病毒,主要是RV(45.60%,173/379)和NV(14.20%,54/379)。混合感染26例(11.40%),以RV与和NV组合占首位(50.00%,13/26)。
我国RV腹泻监测网全年系统监测结果表明,5岁以下住院腹泻患儿的RV中位检出率为46%(范围:16%~61%)[3],本次监测结果(45.6%)与之相符,但远高于我国5岁以下儿童门诊腹泻患儿的RV检出率(29%)[3],说明RV感染的临床症状更严重,住院率更高。
我国东南沿海地区常被认为是NV高发区[4],乌鲁木齐是北方城市,院腹泻患儿中NV检出率为11.4%,和国内北方城市NV研究报道(大约8.9%~10.3%) 较为接近,但是明显低于我国东南部城市[6]。Patel等[7]2008年对13项NV性腹泻的系统性综述研究(大多数是儿童)发现NV感染率为12%(范围:5%~36%),我们的结果与之相近。NV可以通过粪-口途径、污染的水源和食物、空气以及人与人的直接接触等多种途径传播,并具有较高的暴发率[7],所以做好NV的防控工作尤其重要。
SaV感染在世界范围内均有分布,发病率为0.3%~9.3%[8]。中国疾病预防控制中心对我国9省市住院患儿SaV流行情况的调查结果显示,我国急性腹泻患儿SaV总阳性比例仅为0.9%,兰州地区2003—2007年住院患儿急性腹泻患儿阳性率为1.13%,香港2008年的一项调查中SaV感染率仅约为1%[9],这些与我们的研究结果(1.1%)较为一致。
本次监测结果中混合感染包括5种组合,检出率达到6.9%。希腊、法国、德国等欧洲国家以往的报道结果显示混合感染率范围为4.4%~29.0%[10];我国兰州地区曾报道混合感染率为3.9%[11]。RV是混合感染中最常见的病毒,并以RV和NV组合所占比例最大(50.0%),德国[12]、日本[13]等国家报道也是如此。本次研究中未发现3种或者以上病原同时感染的情况。虽然目前病毒之间的相互组合对疾病严重程度是否有增强作用尚存争议[14], 但是混合感染的存在已经是一个不容忽视的问题。我们应该更加重视并将混合感染情况纳入流行病学监测以及临床病理学研究之中。
RV感染呈晚秋和冬季流行,在温暖季节最低,和其他研究基本相似[15]。NV具有和RV相似的流行特征,也多在秋冬季流行。日本[16]、加拿大[17]等国及中国北方城市如北京、兰州、天津等地NV也常在秋冬季节或者早春流行 ,但在一些不同的欧洲国家NV呈春夏季节流行模式[18],我国Zheng等[6]的研究也证明我国南方城市杭州、上海和重庆的NV流行自4月开始活跃,通常在夏秋季出现流行高峰。由此说明,NV的流行季节特征有明显的地区差异,地理位置、气候条件以及流行株的不同可能是NV流行季节出现差异的原因。本研究中AstV感染、AdV和SaV感染未发现明显的季节流行规律,这可能与我们有限的阳性病例(分别只有16、12和4例)有关。
5种病毒感染均无性别差异。病毒性腹泻高发年龄是7~12月龄,2岁以下患儿占98.3%(225/229)。国内外研究提示2岁以下儿童是RV和NV的易感人群 ,本研究中RV以7~12月龄感染率(53.9%)最高,提示低龄儿童应为RV疫苗施治的重点人群。通过比较发现,RV感染平均年龄(9.5±4.4)月龄小于NV平均年龄(12.3±9.6)月龄(P=0.002),支持儿童中NV感染年龄比RV感染年龄偏大的观点[6]。AstV感染平均年龄为(11.8±9.4)月龄,但各年龄组检出率差距较小。AdV和SaV感染全部发生于2岁以下儿童,也与部分研究学者的结论一致[19]。混合感染无特定的年龄分布特点。
本次监测为了解2010年乌鲁木齐住院腹泻患儿中5种常见病毒及其混合感染的流行状况提供了重要的背景资料。
参考文献
[1] Ma L, Gao YJ, Wang ZJ, et al. Analysis of the pathogens in infectious diarrhea (other than cholera, dysentery, typhoid and paratyphoid) cases reported in China in 2009[J]. Chinese Journal of Microecology,2010,22(7):658-661, 665. (in Chinese) 马莉,高永军,王子军,等. 2009年全国其他感染性腹泻报告病例分析[J]. 中国微生态学杂志,2010,22(7):658-661, 665.
[2] Dennehy PH. Viral gastroenteritis in children[J]. Pediatr Infect Dis J,2011,30(1):63-64.
[3] Zhang LJ, Fang A. Development on the epidemiology and disease burden of rotavirus in China[J]. Chinese Journal of Vaccines and Immunization,2007,13(2):186-191. (in Chinese) 张丽杰,方安.中国婴幼儿轮状病毒腹泻的流行病学和疾病负担研究进展[J]. 中国疫苗和免疫,2007,13(2):186-191.
[4] Guo L, Song J, Xu X, et al. Genetic analysis of norovirus in children affected with acute gastroenteritis in Beijing,2004-2007[J]. J Clin Virol,2009,44(1):94-98.
[5] Xu J, Yang Y, Sun J. Molecular epidemiology of norovirus infection among children with acute gastroenteritis in Shanghai, China,2001-2005[J]. J Med Virol,2009,81(10):1826-1830.
[6] Zheng M, Chen J, Gong ST, et al. Epidemiological surveillance of norovirus and rotavirus diarrhea among outpatient children in five metropolitan dties[J]. Chin J Pediatr,2010,48(8):564-570.
[7] Patel MM, Widdowson MA, Glass RI, et al. Systematic literature review of role of noroviruses in sporadic gastroenteritis[J]. Emerg Infect Dis,2008,14(8):1224-1231.
[8] Sdiri-Loulizi K, Hassine M, Gharbi-Khelifi H, et al. Molecular detection of genogroup Ⅰ sapovirus in Tunisian children suffering from acute gastroenteritis[J]. Virus Genes,2011,43(1):6-12.
[9] Li CS, Chan PK, Tang JW. Prevalence of diarrhea viruses in hospitalized children in Hong Kong in 2008[J]. J Med Virol,2009,81(11):1903-1911.
[10] Tran A, Talmud D, Lejeune B, et al. Prevalence of rotavirus, adenovirus, norovirus, and astrovirus infections and coinfections among hospitalized children in northern France[J]. J Clin Microbiol,2010,48(5):1943-1946.
[11] Jin Y, Cheng WX, Yang XM, et al. Viral agents associated with acute gastroenteritis in children hospitalized with diarrhea in Lanzhou, China[J]. J Clin Virol,2009,44(3):238-241.
[12] Oh DY, Gaedicke G, Schreier E. Viral agents of acute gastroenteritis in German children: prevalence and molecular diversity[J]. J Med Virol,2003,71(1):82-93.
[13] Nakanishi K, Tsugawa T, Honma S, et al. Detection of enteric viruses in rectal swabs from children with acute gastroenteritis attending the pediatric outpatient clinics in Sapporo, Japan[J]. J Clin Virol,2009,46(1):94-97.
[14] Liu C, Grillner L, Jonsson K, et al. Identification of viral agents associated with diarrhea in young children during a winter season in Beijing, China[J]. J Clin Virol,2006,35(1):69-72.
[15] Kittigul L, Pombubpa K, Taweekate Y, et al. Molecular characterization of rotaviruses, noroviruses, sapovirus, and adenoviruses in patients with acute gastroenteritis in Thailand[J]. J Med Virol,2009,81(2):345-353.
[16] Dey SK, Phathammavong O, Okitsu S, et al. Seasonal pattern and genotype distribution of norovirus infection in Japan[J]. Pediatr Infect Dis J, 2010,29(5):e32-e34.
[17] Levett PN, Gu M, Luan B, et al. Longitudinal study of molecular epidemiology of small round-structured viruses in a pediatric population[J]. J Clin Microbiol,1996,34(6):1497-1501.
[18] Oldak E, Sulik A, Rozkiewicz D, et al. Norovirus and Rotavirus-two major causative agents of sporadic viral gastroenteritis in hospitalized Polish children[J]. Adv Med Sci,2009,54(2):183-186.
[19] Chhabra P, Dhongade RK, Kalrao VR, et al. Epidemiological, clinical, and molecular features of norovirus infections in western India[J]. J Med Virol,2009,81(5):922-932.
[2] Dennehy PH. Viral gastroenteritis in children[J]. Pediatr Infect Dis J,2011,30(1):63-64.
[3] Zhang LJ, Fang A. Development on the epidemiology and disease burden of rotavirus in China[J]. Chinese Journal of Vaccines and Immunization,2007,13(2):186-191. (in Chinese) 张丽杰,方安.中国婴幼儿轮状病毒腹泻的流行病学和疾病负担研究进展[J]. 中国疫苗和免疫,2007,13(2):186-191.
[4] Guo L, Song J, Xu X, et al. Genetic analysis of norovirus in children affected with acute gastroenteritis in Beijing,2004-2007[J]. J Clin Virol,2009,44(1):94-98.
[5] Xu J, Yang Y, Sun J. Molecular epidemiology of norovirus infection among children with acute gastroenteritis in Shanghai, China,2001-2005[J]. J Med Virol,2009,81(10):1826-1830.
[6] Zheng M, Chen J, Gong ST, et al. Epidemiological surveillance of norovirus and rotavirus diarrhea among outpatient children in five metropolitan dties[J]. Chin J Pediatr,2010,48(8):564-570.
[7] Patel MM, Widdowson MA, Glass RI, et al. Systematic literature review of role of noroviruses in sporadic gastroenteritis[J]. Emerg Infect Dis,2008,14(8):1224-1231.
[8] Sdiri-Loulizi K, Hassine M, Gharbi-Khelifi H, et al. Molecular detection of genogroup Ⅰ sapovirus in Tunisian children suffering from acute gastroenteritis[J]. Virus Genes,2011,43(1):6-12.
[9] Li CS, Chan PK, Tang JW. Prevalence of diarrhea viruses in hospitalized children in Hong Kong in 2008[J]. J Med Virol,2009,81(11):1903-1911.
[10] Tran A, Talmud D, Lejeune B, et al. Prevalence of rotavirus, adenovirus, norovirus, and astrovirus infections and coinfections among hospitalized children in northern France[J]. J Clin Microbiol,2010,48(5):1943-1946.
[11] Jin Y, Cheng WX, Yang XM, et al. Viral agents associated with acute gastroenteritis in children hospitalized with diarrhea in Lanzhou, China[J]. J Clin Virol,2009,44(3):238-241.
[12] Oh DY, Gaedicke G, Schreier E. Viral agents of acute gastroenteritis in German children: prevalence and molecular diversity[J]. J Med Virol,2003,71(1):82-93.
[13] Nakanishi K, Tsugawa T, Honma S, et al. Detection of enteric viruses in rectal swabs from children with acute gastroenteritis attending the pediatric outpatient clinics in Sapporo, Japan[J]. J Clin Virol,2009,46(1):94-97.
[14] Liu C, Grillner L, Jonsson K, et al. Identification of viral agents associated with diarrhea in young children during a winter season in Beijing, China[J]. J Clin Virol,2006,35(1):69-72.
[15] Kittigul L, Pombubpa K, Taweekate Y, et al. Molecular characterization of rotaviruses, noroviruses, sapovirus, and adenoviruses in patients with acute gastroenteritis in Thailand[J]. J Med Virol,2009,81(2):345-353.
[16] Dey SK, Phathammavong O, Okitsu S, et al. Seasonal pattern and genotype distribution of norovirus infection in Japan[J]. Pediatr Infect Dis J, 2010,29(5):e32-e34.
[17] Levett PN, Gu M, Luan B, et al. Longitudinal study of molecular epidemiology of small round-structured viruses in a pediatric population[J]. J Clin Microbiol,1996,34(6):1497-1501.
[18] Oldak E, Sulik A, Rozkiewicz D, et al. Norovirus and Rotavirus-two major causative agents of sporadic viral gastroenteritis in hospitalized Polish children[J]. Adv Med Sci,2009,54(2):183-186.
[19] Chhabra P, Dhongade RK, Kalrao VR, et al. Epidemiological, clinical, and molecular features of norovirus infections in western India[J]. J Med Virol,2009,81(5):922-932.
|
扩展功能
|
|
| 本文信息 | |
| PDF全文 | |
| HTML全文 | |
| 参考文献 | |
| 服务与反馈 | |
| 加入引用管理器 | |
| 引用本文 | |
| Email Alert | |
| 本文作者相关文章 | |
| 沙比热木·托合塔木 | |
| 阿依古丽·伊尔哈力 | |
| 刘红斌 | |
| 毋跃文 | |
| 李新兰 | |
| PubMed | |
| Article by Sabiremu Tuohetamu | |
| Article by Ayiguli Yerhali | |
| Article by LIU Hong-bin | |
| Article by WU Yue-wen | |
| Article by LI Xin-lan | |